



[Product Collection] 03 Simulation Model – Left Atrial Appendage Occlusion Heart Model | Precise Deployment for Intuitive Evaluation
Release date:
2025-08-28 15:50
Atrial fibrillation (AF) is a common cardiac arrhythmia seen in clinical practice, affecting over 40 million patients worldwide. During AF, blood flow within the left atrial appendage becomes sluggish, increasing the risk of clot formation. If these clots dislodge, they can travel to the brain, leading to stroke—a condition with extremely high rates of disability and mortality. Left atrial appendage closure has emerged as a critical strategy for preventing stroke in AF patients. This procedure involves placing a closure device into the left atrial appendage, effectively blocking the pathway that allows clots to enter the bloodstream. The surgery relies on specialized instruments, including delivery sheaths, guidewires, and dedicated occluders such as the Watchman or LAmbre devices. However, in real-world clinical settings, the left atrial appendage exhibits diverse anatomical shapes—ranging from "chicken-wing" to "cauliflower" or "windsock" types—and is closely situated near critical structures like pulmonary veins and coronary arteries. As a result, ensuring the stability of these devices in the complex intracardiac environment and achieving optimal apposition of the occluder during surgery remain challenging tasks that are difficult to predict preoperatively. Additionally, the varying sizes and irregular inner surfaces of the left atrial appendage mean that improper handling during the procedure could easily lead to serious complications, such as pericardial tamponade or device displacement—both of which demand exceptional spatial awareness and precise instrument control from the surgeon. Traditional training methods often fall short in replicating the true anatomical variations and surgical risks involved, making the development of realistic left atrial appendage closure heart models essential for overcoming these technical hurdles.
Surgical procedure
Atrial fibrillation (AF) is a common clinical arrhythmia affecting over 40 million patients worldwide. During AF, blood flow in the left atrial appendage becomes sluggish, increasing the risk of clot formation. If these clots dislodge, they can travel to the brain, leading to stroke—a condition with extremely high rates of disability and mortality. Left atrial appendage closure has emerged as a critical strategy for preventing stroke in AF patients, as it involves placing a device into the left atrial appendage to block off the pathway that allows clots to enter the bloodstream.
Surgery relies on instruments such as delivery sheaths, guidewires, and specialized occluders (e.g., the Watchman Occluder, LAmbre Occluder). However, in clinical practice, the left atrial appendage exhibits diverse anatomical shapes—ranging from "chicken-wing" to "cauliflower" or "windsock" types—and is closely situated near critical structures like pulmonary veins and coronary arteries. As a result, it remains challenging to preoperatively assess the stability of these devices in the complex intracardiac environment, as well as the precise fit of the occluders. Additionally, the variable size and irregular inner surface of the left atrial appendage’s opening increase the risk of complications such as pericardial tamponade or device displacement if procedures are not performed carefully. This places extremely high demands on a physician’s spatial awareness and dexterity in manipulating surgical tools. Traditional training methods often fall short in replicating real-world anatomical variations and associated surgical risks. To address these technical challenges, left atrial appendage closure heart models have emerged as a reliable solution, offering an effective platform for mastering this intricate procedure.
Structure
Thoracic aorta + abdominal aorta + peripheral vessels (hepatic artery + renal artery + splenic artery + superior mesenteric artery) + lower limb arteries (popliteal artery, anterior tibial artery, posterior tibial artery, peroneal artery) + bilateral upper limb arteries (subclavian artery + axillary artery + brachial artery + radial artery)
Superior vena cava + right heart + pulmonary artery + inferior vena cava + renal veins + lower limb veins (popliteal vein, anterior tibial vein, posterior tibial vein, fibular vein) + bilateral upper limb veins (subclavian vein + axillary vein + brachial vein + radial vein)
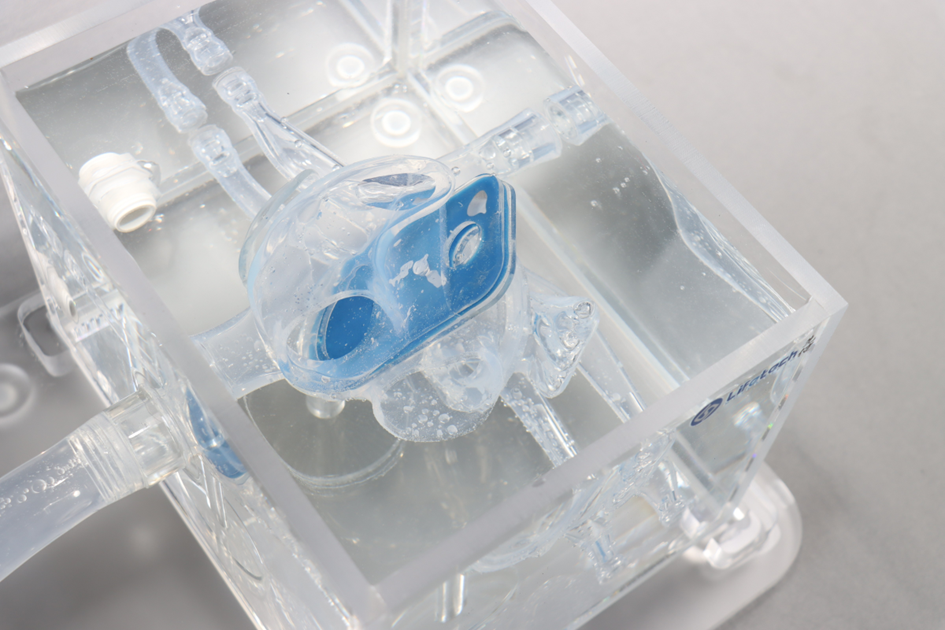
The left atrial appendage occlusion heart model is crafted from medical-grade, highly elastic, bio-inspired silicone material, accurately replicating the soft texture and mechanical properties of cardiac tissues—particularly the delicate structure and elasticity of the left atrial appendage wall. Utilizing 3D modeling technology driven by medical imaging data, the model faithfully recreates the left atrium, left atrial appendage, and their surrounding anatomical structures at a 1:1 scale. It meticulously captures intricate anatomical details, such as the pectinate muscles and lobulated features of the left atrial appendage, while also featuring interchangeable modules that represent various typical appendage shapes—like the "chicken-wing" and "cauliflower" types.
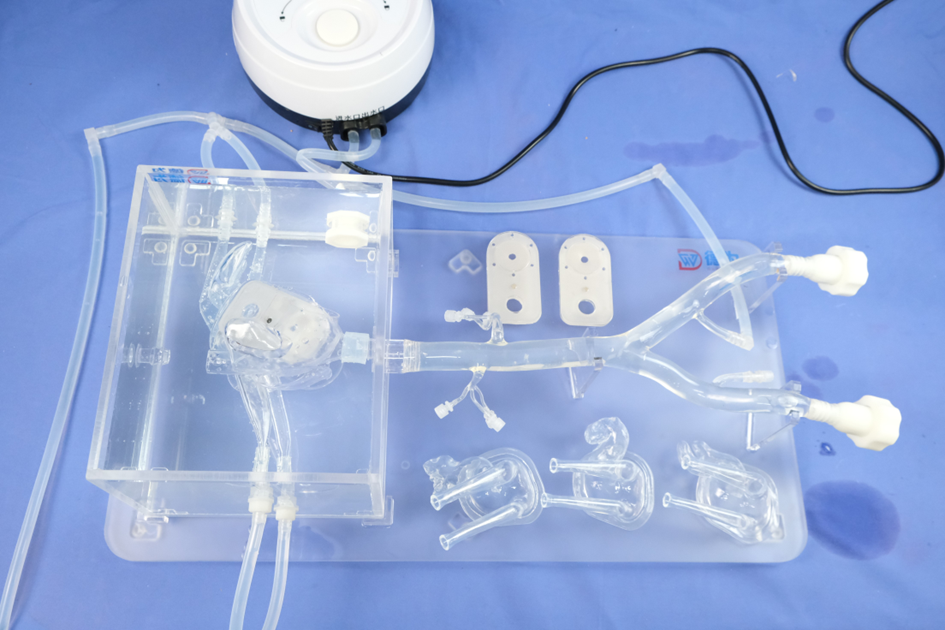
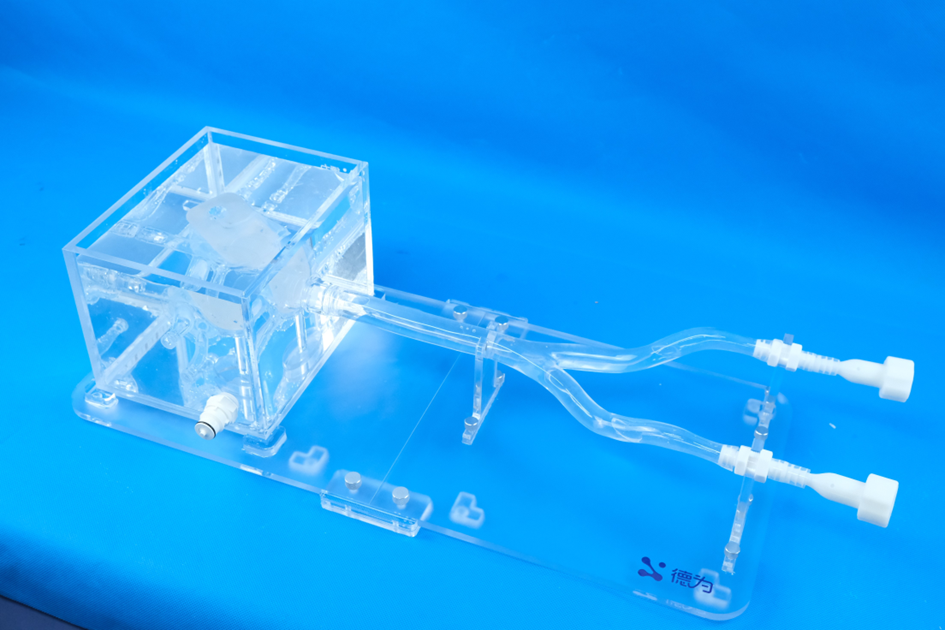
The model can be paired with a simulated circulatory system, allowing users to adjust blood flow velocity and pressure while realistically mimicking the stagnant blood flow conditions typically observed in the left atrial appendage during atrial fibrillation. Additionally, its device interface is fully compatible with mainstream clinical left atrial appendage closure devices. Thanks to a specially designed fixation mechanism, the system ensures stable and lifelike handling of the delivery sheath and occluder during simulated procedures, creating a highly realistic environment ideal for surgical training.
Functions and Applications
This model focuses on end-to-end simulation training for left atrial appendage closure procedures: Physicians can repeatedly practice techniques such as precisely locating the atrial septal puncture site, mastering the delicate maneuvers of advancing and rotating the delivery sheath, accurately deploying the occluder device, and performing tension-testing protocols—gaining expert proficiency in assessing the occluder’s sealing and stability. Whether medical students are learning the fundamentals of LAA closure, clinicians preparing for complex cases through pre-procedural simulations, or device manufacturers testing the performance of new products, this model delivers standardized, highly repeatable training scenarios.
The left atrial appendage occlusion heart model is widely used in medical practice and research. In the field of surgical training, it realistically simulates the complex anatomy of the left atrial appendage and the overall cardiac structure, providing physicians with a platform for repeated practice. This allows them to master critical procedures such as atrial septal puncture and occluder deployment, significantly reducing risks during actual surgeries—making it especially ideal for novice doctors to build up their experience.
In the equipment R&D and testing phase, the model can be used to evaluate the fit, stability, and safety of different types of occluders. Researchers simulate various left atrial appendage shapes on the model to assess the anchoring performance and wall-apposition accuracy of the occluders, enabling them to refine the device design and drive innovation and improvement in next-generation occluders.
In clinical decision-making support, patient-specific heart models tailored from individualized imaging data enable doctors to visually assess the morphology of the left atrial appendage, select the most appropriate occluder device, plan the surgical approach, and anticipate potential intraoperative challenges—thereby enhancing the success rate of the procedure. Additionally, these models can be used in medical education and patient communication: they help medical students grasp surgical principles, while also allowing physicians to clearly explain the procedure and expected outcomes to patients and their families, ultimately improving doctor-patient communication.
Keywords:
Other news
Request a quote
*Please keep your phone accessible—we'll reach out to you within 24 hours.
PARTNERSHIP
Partnership

Contact us
Address: Wangzuo Qujiang, 3269 Yanxiang Road, Yanta District, Xi'an City
Pre-sales Consultation
Request a quote




